If you’ve been getting semaglutide through a telehealth company at $100–$200 a month, you need to read this. The rules have changed, enforcement is escalating, and the landscape looks different today than it did a year ago.
Before compounded options get harder to access, it’s worth knowing where you stand — check your eligibility for the branded medications.
Why Compounded Semaglutide Existed in the First Place
Starting in 2022, Ozempic and Wegovy demand exploded faster than Novo Nordisk could manufacture them. The FDA placed both drugs on its official Drug Shortage List — and that designation opened a legal door.
Federal law allows compounding pharmacies to produce versions of drugs that are in shortage. So thousands of smaller pharmacies and telehealth platforms started making compounded semaglutide: the same active ingredient, made in-house or through specialized compounders, sold at a fraction of brand-name prices. For many people, this was the only realistic way to access GLP-1 therapy.
At its peak, compounded semaglutide was generating an estimated $1 billion per year for the compounding market, with hundreds of thousands of Americans relying on it.
The Shortage Ended. Then Things Got Complicated.
On February 21, 2025, the FDA officially declared the semaglutide shortage resolved. Novo Nordisk stated it was now meeting or exceeding U.S. demand.
That declaration started a countdown. The FDA gave:
- State-licensed (503A) compounding pharmacies until April 22, 2025 to stop producing compounded semaglutide that was “essentially a copy” of Ozempic or Wegovy
- Larger outsourcing facilities (503B) until May 22, 2025
The stated reason: once a drug is no longer in shortage, the legal justification for compounding copies of it disappears.
What happened next was not what the FDA expected.
Companies Didn’t Stop — They Found Workarounds
After the deadlines passed, compounded semaglutide prescriptions actually increased, according to research firm IQVIA’s October 2025 report. Companies found a loophole: federal law allows compounding of a customized version of a drug when a licensed provider determines the modification makes a “clinical difference” for the patient.
The most common workaround? Adding B vitamins — usually B12 or B6 — to the compound. The argument: the added vitamins reduce GLP-1 side effects, making it a distinct formulation rather than a copy.
By late 2025, approximately 80% of compounded semaglutide prescriptions included supplemental ingredients, according to the IQVIA report. Hims & Hers — one of the largest telehealth platforms — publicly leaned into this strategy, with CEO Andrew Dudum stating compounded versions would be available “indefinitely” through personalized formulations.
The 2026 Crackdown Is Real
The FDA didn’t accept the B-vitamin argument quietly.
In February 2026, when Hims & Hers announced it would also offer a compounded oral semaglutide pill, the response was swift. The Department of Health and Human Services asked the DOJ to investigate the company for potential violations of the Food, Drug, and Cosmetic Act. The FDA announced it would take “decisive steps” to restrict compounded GLP-1s being mass marketed as equivalent to FDA-approved drugs.
Hims backed down on the pill within days — only for Novo Nordisk to file a patent infringement lawsuit anyway. Hims stock dropped 35% in a week.
As of March 2026, the FDA crackdown is ongoing. Enforcement is specifically targeting:
- Companies mass-producing compounds under the guise of “personalized” dosing
- Pharmacies sourcing active pharmaceutical ingredients from facilities not registered with the FDA
- Products using salt forms of semaglutide (like semaglutide acetate or semaglutide sodium) rather than the base form — which the FDA considers unapproved new drugs, not compounded versions of an approved one
- Counterfeit products labeled with the names of pharmacies that didn’t actually compound them
The FDA has received over 455 adverse event reports linked to compounded semaglutide. Many involved dosing errors — patients measuring incorrect doses from vials — leading to hospitalizations in some cases.
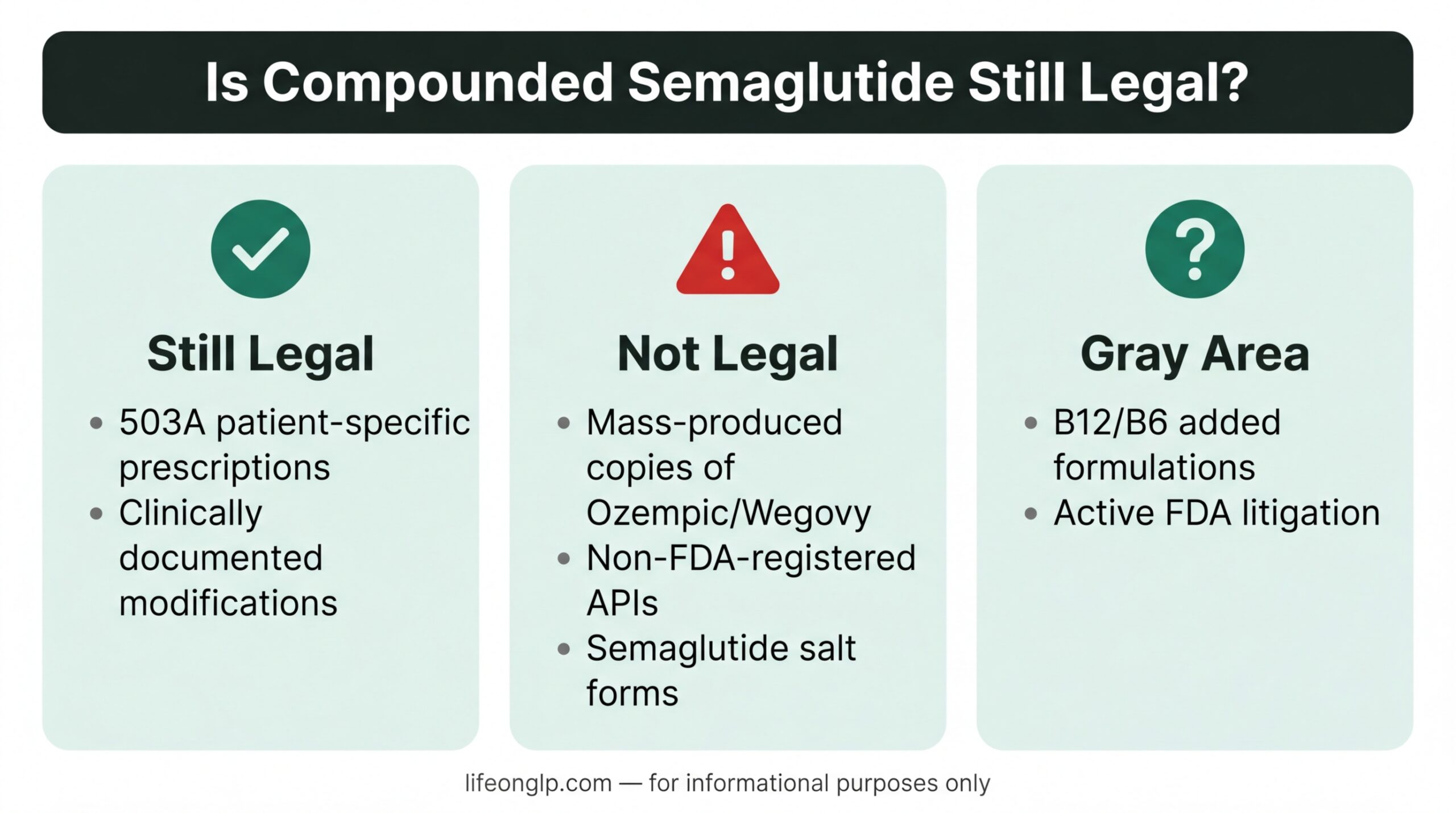
So Is Compounded Semaglutide Still Legal?
It depends on the pharmacy and the prescription.
Still legal (for now):
- Patient-specific prescriptions from 503A pharmacies, where a provider documents a clinical reason the standard brand-name drug doesn’t meet the patient’s needs
- Formulations with documented, clinically meaningful modifications (this is contested territory)
Not legal:
- Mass production of “essentially a copy” of Ozempic or Wegovy without a shortage-based justification
- Products with non-FDA-registered APIs
- Salt forms of semaglutide sold as equivalent to the semaglutide in Ozempic/Wegovy
Gray area:
- B12/B6 additions — the FDA hasn’t explicitly ruled these out as a basis for compounding, but it’s increasingly skeptical, and both Novo Nordisk and Eli Lilly are aggressively litigating against this practice
The Outsourcing Facilities Association (OFA) — an industry group — has been suing the FDA to block enforcement, arguing the shortage declaration was premature. As of early 2026, that litigation is ongoing and could affect timelines.
What This Means for People Currently on Compounded Semaglutide
If you’re getting compounded semaglutide through a reputable telehealth platform:
You may not see an immediate disruption. Major platforms are navigating the legal gray area and haven’t shut down. But the ground is shifting. Check your provider’s communications and be aware that what’s available today may not be available in 6 months.
If your platform suddenly stops offering it:
This has already happened to some smaller operators. According to STAT News, several smaller telehealth companies shut down compounded GLP-1 services after the FDA’s escalation in early 2026.
If you’re paying under $200/month through a compounding route:
Start researching your alternatives now, not when your supply runs out. The options below are imperfect, but they exist.
Your Realistic Alternatives Right Now
Brand-Name Wegovy Through Direct-Pay Programs
Novo Nordisk has a self-pay program (NovoCare) that can bring Wegovy to around $199/month for cash-paying patients. This is a significant price drop from the list price of $1,300+, driven in part by competition from the compounding market.
The New Oral Wegovy Pill
The FDA approved an oral semaglutide pill (brand-name Wegovy in pill form) in December 2025 — the first GLP-1 to come in a swallowable tablet. Cash-pay pricing starts around $149/month in some programs, making it the lowest entry point currently available for an FDA-approved GLP-1 weight loss medication.
Telehealth Partners Offering Brand-Name GLP-1s
Platforms like Ro (partnered with Eli Lilly since 2024) and Hims & Hers (now partnered directly with Novo Nordisk for Wegovy) have pivoted toward offering brand-name medications alongside or instead of compounded versions. This is worth checking if you’re already using these platforms.
Tirzepatide (Mounjaro/Zepbound) Options
The tirzepatide compounding situation is slightly different — and in some ways, even more restrictive. But Eli Lilly’s direct-pay program offers Zepbound at $299–$449/month, and clinical data shows it may produce greater weight loss than semaglutide-based options for many patients.
Insurance Appeal
If you’ve been denied insurance coverage for weight loss, it’s worth re-appealing. Reddit communities like r/Ozempic and r/semaglutide have shared appeal letter templates that have worked. Some plans now cover GLP-1s for patients with BMI over 40, or with documented weight-related conditions like sleep apnea, hypertension, or pre-diabetes.
What to Watch in the Coming Months
The legal battle between compounders and the FDA — and between brand-name manufacturers and telehealth platforms — is far from over. A few things to track:
- OFA v. FDA (federal court in Texas): The ongoing lawsuit challenging the FDA’s shortage resolution. A ruling here could change enforcement timelines.
- Hims & Hers vs. Novo Nordisk: The patent lawsuit filed in February 2026 is ongoing and could reshape how personalized compounding is defined legally.
- Generic semaglutide outside the US: India’s semaglutide patent expired in early 2026, triggering launches from major generic manufacturers at prices as low as $8 per injection. This won’t directly affect US access under current law, but it adds pressure on Novo Nordisk to keep self-pay prices competitive.
The Bottom Line
The era of cheap, freely available compounded semaglutide is narrowing — not gone yet, but under serious legal and regulatory pressure.
If you’re currently on compounded semaglutide and it’s working for you: keep taking it, stay in contact with your provider, and start building a backup plan. If your platform goes quiet or changes its offering, move quickly — there are now more legitimate lower-cost alternatives than there were a year ago.
The medication works. The path to accessing it is just getting more complicated.
The information in this article is for educational purposes only and does not constitute medical or legal advice. Always consult with a licensed healthcare provider before making any changes to your medication.
Some links on this site may be affiliate links. This does not affect the editorial content or our recommendations.